Reid
You can download a PDF version of this article here
I apologise if there is a little overlap with Belinda’s presentation, but perhaps you could think of hers as the ‘sacred’ and of mine as the ‘profane’. I am not speaking this evening as Medical Director of the Medical Council; the views expressed are mostly my own.
Some history
My version of history will be a little bit different from Belinda’s. I will take you through the new order, particularly as it applies in NSW. I am going to go right back in history because I think it is interesting and relevant – right back to the colonisation of NSW in 1788. At that time, things were pretty bawdy around Sydney Cove. This is a famous portrait of Black-Eyed Sue with a gin bottle.

Her friend Sweet Poll doesn’t look too sweet with that significant wardrobe malfunction. Nevertheless, the picture depicts their menfolk saying goodbye from Plymouth as they were about to avoid the gallows on the hill and be transported to NSW.
It was people like that who formed the initial population of the colony. As a result, law and order was really not well maintained for quite a long period of time and a particular problem was individuals holding themselves out to be surgeons and getting up to all sorts of nonsense within the colony, so very early in the colony’s history, in 1837, the Medical Board was established. It wasn’t the oldest Medical Board in the country. Tasmania had even more problems and they had established their Medical Board the year before. It might interest you to know that the Medical Board in NSW is the second oldest medical board in the world. It predates the UK General Medical Council by some 20 years, a fact which the GMC is rather unwilling to acknowledge, thinking that they are rather wonderful.
I have often wondered about the reason for that. I suspect it was because they had exported their felons to NSW and our need was perhaps more urgent than theirs in establishing some system of regulation.
Since Federation in 1901, there were several attempts at creating a national registration system – in 1918, 1937 and again in 1959. All failed for various reasons, some being similar to more recent attempts. Essentially the pace of change in developing a national system of medical regulation was glacial.
Mutual recognition
The more recent history of national registration begins in 1992 with the Mutual Recognition Act, with which many of you will be familiar. Prior to July 2010, it enabled us to adopt action taken by one state in another state without having to go through another process. If a doctor had had conditions imposed on his registration for some disciplinary reason, for example, in Queensland, and wanted to work in NSW, we could, as well as demanding a fee, impose the same conditions as in Queensland without any particular process.
Interestingly, mutual recognition was not developed for this purpose. It was actually developed for commercial purposes, such as ensuring that the quality and standards of sausages and beer were consistent around the country. Somebody eventually had the ‘good idea’ that you could apply this to professional regulation as well. It never quite worked as well as perhaps it could have, because it was really not developed for regulation. Nevertheless it has served us reasonably well for nearly two decades.
National registration
In 2003, the medical boards around the country decided that national registration was something they really ought to start to look at and to pursue – because if they didn’t, somebody else would. A lot of work went into thinking about how such a scheme could operate. The model we favoured – and I was involved in the discussions at that time – was the ‘driver’s licence’ model. You could be registered in one jurisdiction and, without any activity on your part, you could take yourself to another and, provided you abided by the law, you could drive (or practise) there as well.
It was envisaged that this model would also ensure that people with particular issues with their registration by way of conditions wouldn’t be able to move from jurisdiction to jurisdiction without the knowledge of the receiving state. The driver’s licence model would apply for the majority of practitioners. Time and other events overtook us. Because the IT solution to support that system was very slow in development, that initiative didn’t ever reach fruition and was overtaken by the Productivity Commission’s report in 2005.
The Productivity Commission
The Productivity Commission, we all thought at the time, was probably a little bit of a joke – who ever commenced anything that the Productivity Commission recommended? Essentially, their recommendation was what I call a ‘fishing licence’ model. I say that rather disrespectfully, because the Productivity Commission didn’t really understand that professional regulation is different from buying a fishing licence every year – that it is a much more complex process and that there are many considerations in terms of fitness to practise. It is not just a matter of paying your fee and getting your licence – but that was the simplicity of the Productivity Commission’s model.
COAG
That puddled around for a while, eventually being taken up by the Council of Australian Governments, with directions that eventually lead to the establishment of the national registration scheme which Belinda has so ably described. Belinda has listed why we would have national registration. My list is a little different.
Why national registration?
Because we are one nation – that is pretty obvious. Achieving national registration was by no means the slowest evolution in this country. You have only to look at things like the Indian-Pacific railway, which the Governor of NSW, Charles Fitzroy, decided in 1848 would be a really good idea – with a standard gauge railway enabling trains to move from one side of the country to the other. It took from 1848 until 1970 for that to occur. Because of the different gauge railways in every state, travel from Perth to Sydney involved changing trains seven times. I guess that it is not such a surprise that it took such a long time for national registration, even though we are one nation, but one nation under Federation.
Workforce mobility, flexibility and sustainability are laudable goals of the new scheme, with uniformity of law, best practice and reduction of red tape. However, many of us believe right now that there is no demonstrable reduction in red tape; in fact, some frustrating red tape still needs to be dealt with.
Workforce controls?
Many people would also have been concerned about issues like workforce control, particularly in the early iterations of the scheme, where it was imagined that there would be a single board for all professions, not ten boards, each profession having its own board. The initial proposal was for a single board covering all health professions. Many people thought that that was the beginning of a slippery slope towards workforce substitution and blurring of the boundaries between the various professional groups. I guess time will tell.
‘One size fits all’
Belinda has also gone into the details of which professions are covered. Essentially, the new scheme is a ‘one size fits all’ scheme for all professions. It is a single piece of legislation which applies (other than in NSW, which I discuss below) which applies equally to all health professions.
NSW the exception
NSW has opted out of everything but the registration functions. It manages its own complaints, health matters, performance and conduct issues under its own legislation. That legislation is actually embedded in the national legislation. There is now a single piece of legislation, but a part of that legislation applies only in NSW, so there is a single national law with the NSW bit embedded in it.
Why did we opt out of these aspects of the new scheme? Mainly because there was such broad-based local support for our co-regulatory model with the Health Care Complaints Commission.
The scheme, as it exists now in every other jurisdiction, has the investigatory and prosecutory functions embedded within the national board and its local boards and offices of Australian Health Practitioner Regulation Agency (AHPRA). This means that, when a complaint in received in all the other states, the Board will receive the complaint, assess the complaint, decide whether or not to investigate the complaint, investigate the complaint, decide whether or not to prosecute the complaint, prosecute the complaint and determine the penalty.
NSW abandoned that model in 1992 after the Chelmsford Inquiry and adopted the co-regulatory system that we now have. This ensures that, if a matter requires investigation and proceeds through to prosecution, it is managed by the Health Care Complaints Commission with points of consultation with the Board, as it used to be, but essentially with independence. We have always believed, at least since we have had this arrangement in place, that it is a jurisprudentially sound system.
Why NSW opted out
Various people in NSW argued very strongly for the NSW model to be adopted in the national scheme, but we were overruled by weight of numbers and just because “anything from NSW can’t be good”. Because there was such universal commitment in NSW during the consultation leading up to the national scheme, from all of the boards and very strongly from the community, NSW was exempted from these aspects of the national scheme.
There was also concern, particularly from the NSW Medical Board – perhaps not so much from the other professions – about a ‘lowest common denominator effect’ of the new scheme. The Board felt that it had moved ahead at such a pace in recent years and had been so innovative in developing new programs that we were at the cutting edge in medical regulation around the world. It didn’t want to risk having those programs diminished by the lowest common denominator effect of a new scheme applying to all professions.
Obviously, for many professions in many states, the new scheme is a great improvement on the prior systems they had in place, but we could see, in the lead-up to the national scheme, that that was not necessarily going to be the case in NSW. These are the reasons that NSW opted out.
The design of the new scheme
The design of the system that we have now is not pretty, but it kind of works. We are trying hard to make it work.

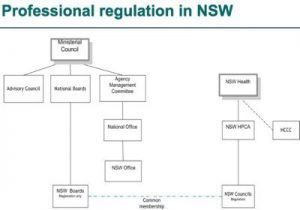
It’s really difficult to illustrate the way things fit together. The simplified chart is not exactly accurate. On the left is the national organisation. The Ministerial Council at the top sits over the ten national boards, each of which can have their state boards – if they have elected to do that. In NSW, that state board is dealing with registration matters only, so it looks at registration of international medical graduates, local graduates, any questions relating to the actual process of registration and renewal of registration. There is a national AHPRA office and there is a NSW AHPRA office.
On the right are the regulatory systems: NSW Health and a new organisation, the Health Professional Councils Authority (HPCA). All professions in NSW have been brought together under this one umbrella. Then there are the separate councils: the Medical Council, the Nursing Council, the Physiotherapy Council etc; and the HCCC still sits off to the side of NSW Health.
Medical regulation
Let’s just talk about medicine. We now have the National Board – the Medical Board of Australia. We have the “NSW Board of the National Board” and we have the NSW Medical Council, responsible for all the regulatory functions, (performance, conduct and health). We have common membership of those two NSW bodies: the NSW Board of the National Board meets to talk about secret registration business and then exchange hats and become the NSW Medical Council dealing with regulatory issues under specific NSW legislation. That’s how it (kind of) works in NSW.
A lower fee for NSW doctors
One of the other consequences of NSW’s opting out is that our registration fee is less. The national fee for medical practitioners is $650. There is a rebate for NSW practitioners because the NSW Government funds the Health Care Complaints Commission. In all other jurisdictions, the national agency will undertake investigative and prosecutory functions and have the expenses involved in those, which in NSW are funded from a different source. So the fee in NSW is $465, instead of $650.
Many of you who are medically qualified would have received your registration renewal papers recently because many people have registration due on the 30th of this month. You might be mystified as to why your fee is a little less than everybody else’s. It will be interesting to see whether some people will decide that they belong in NSW once they realise that our fees are lower.
Our challenges
Our biggest challenge at the moment is the interface between the Council and the national body. Essentially the Council’s work has not changed. The new legislation relevant to NSW, as Belinda said, is modelled specifically on our old Medical Practice Act. Everything continues to function pretty much as before, so nothing much has changed in our day-to-day activities. The complication is the interface with the national body. I guess that we will, over time, resolve some of the data transfer and IT problems. I’m sure that many of the goals Belinda mentioned will be met. Meanwhile, it is a challenge for all of us.
About Reid
Alison Reid, Medical Director of the Medical Council of NSW, is involved in all aspects of the Council’s work. She overseas the Council’s health and performance programs and is responsible for the initial assessment of complaints.
Alison is a medical graduate of the University of Tasmania. She holds a Master’s Degree in Health Administration from the University of NSW and is a Fellow of the Australasian Faculty of Public Health Medicine. Prior to her current appointment with the Council, Alison spent six years as chief executive of the 1,400-bed Prince of Wales Hospital in Hong Kong, and was Associate Professor of Community Medicine at the Chinese University of Hong Kong. Before that, she was Director of State-Wide Health Services and Director of Public Health in Tasmania.